Wednesday, December 23, 2020
Wednesday, November 11, 2020
The dorsal column–medial lemniscus pathway
The dorsal column–medial lemniscus pathway (DCML) (also known as the posterior column-medial lemniscus pathway, PCML) is a sensory pathway of the central nervous system that conveys sensations of fine touch, vibration, two-point discrimination, and proprioception(position) from the skin and joints. It transmits information from the body to the primary somatosensory cortex in the postcentral gyrus of the parietal lobe of the brain.
The pathway receives information from sensory receptors (missner’s corpuscle, pacinian corpuscle etc.) throughout the body, and carries this in nerve tracts in the white matter of the dorsal columns of the spinal cord to the medulla, where it is continued in the medial lemniscuses, on to the thalamus and relayed from there through the internal capsule and transmitted to the somatosensory cortex.
The name dorsal-column medial lemniscus comes from the two structures that carry the sensory information: the dorsal columns of the spinal cord, and the medial lemniscus in the brainstem.
There are three groupings of neurons that are involved in the pathway: first-order neurons, second-order neurons, and third-order neurons.
The first-order neurons are sensory neurons located in the dorsal root ganglia, that send their afferent fibers through the two dorsal columns – the gracile fasciculus, or gracile tract, and the cuneate fasciculus, or cuneate tract. The first-order axons make contact with second-order neurons of the dorsal column nuclei (the gracile nucleus and the cuneate nucleus) in the lower medulla.
The second-order neurons send their axons to the thalamus.
The third-order neurons are in the ventral nuclear group in the thalamus and fibres from these ascend to the postcentral gyrus.
Sensory information from the upper half of the body is received at the cervical level of the spinal cord and carried in the cuneate tract, and information from the lower body is received at the lumbar level and carried in the gracile tract. The gracile tract is medial to the more lateral cuneate tract.
The axons of second-order neurons of the gracile and cuneate nuclei are known as the internal arcuate fibers and when they cross over the midline, at the sensory decussation in the medulla, they form the medial lemniscus which connects with thalamus; the axons synapse on neurons in the ventral nuclear group which then send axons to the postcentral gyrus in the parietal lobe. All of the axons in the DCML pathway are rapidly conducting, large, myelinated fibers.
Tuesday, November 10, 2020
Lateral spinothalamic tract
The lateral spinothalamic tract, also known as the lateral spinothalamic fasciculus, is an ascending pathway located anterolaterally within the peripheral white matter of the spinal cord. It is primarily responsible for transmitting pain and temperature as well as coarse touch.
The anterior spinothalamic tract (discussed separately), in contrast, primarily transmits coarse touch and pressure.
First-order neurons, whose cell bodies are in the dorsal root ganglion and whose axons extend from peripheral receptors, enter the cord via dorsal nerve roots.
First-order neurons synapse with second-order neurons whose bodies are located in the ipsilateral substantia gelatinosa of dorsal horn of the spinal cord.
The lateral spinothalamic tract then ascends in the lateral funiculus, just medial to the ventral spinocerebellar tract. Fibers of this tract are somatotopically organized for their entire course.
Upon reaching the brainstem, the lateral and anterior spinothalamic tracts combine to form the spinal lemniscus, which runs lateral to the medial lemniscus
The spinal lemniscus terminates in the ventral posterior nucleus of the thalamus. Here, it synapses with third-order neurons, which project to the primary somatosensory area on the ipsilateral side of the cerebral cortex.
Lesion :

Contra-lateral loss of pain & thermal sensibilities below the level of the lesion
Unable to sense pin prick or recognize hot or cold objects
Monday, November 9, 2020
Summary of Somatosensory pathways: lateral & anterior spinothalamic tract and tract of gall and cuneatus
Summary of Somatosensory pathways
The somatosensory system is a part of the sensory nervous system.
It is a complex system of sensory neurons and neural pathways that responds to changes at the external environment or inside the body.
The axons (as afferent nerve fibers) of sensory neurons has two part peripheral and center part. Terminal portion of peripheral portion of axon of sensory neuron is converted into receptors.
Sensory receptors are found all over the body including the skin, epithelial tissues, muscles, bones and joints, internal organs, and the cardiovascular system.
Touch is a crucial means of receiving information. This photo shows tactile markings identifying stairs for visually impaired people.
Somatic senses are sometimes referred to as somesthetic senses, with the understanding that somesthesis includes the sense of touch, proprioception (sense of position and movement), and (depending on usage) haptic perception
The mapping of the body surfaces in the brain is called somatotopy. In the cortex, it is also referred to as the cortical homunculus. This brain-surface ("cortical") map is not immutable, however. Dramatic shifts can occur in response to stroke or injury.
Our nervous system deal two types of sensation conscious and unconscious . this article summarized the main somatosensory pathways|
Topics |
Lateral spino-thalamic tract |
Anterior spinothalamic tract |
Tract of gracilis & cuneatus |
|
Sensation |
Pain and temperature |
Light touch and pressure |
Discriminative touch, vibration , conscious muscle joint sense |
|
Receptor |
Free nerve ending |
Free nerve ending |
Meissners corpuscles, pacinian corpuscles, muscle spindles , tendon organ |
|
1st order neuron |
Posterior root ganglion |
Posterior root ganglion |
Posterior root ganglion |
|
2nd order neuron |
Substantia getalinosa |
Substantia getalinosa |
Nuclei gracilis and nuceatus |
|
3rd order neuron |
Ventral posterior lateral nucleus of thalamus |
Ventral posterior lateral nucleus of thalamus |
Ventral posterior lateral nucleus of thalamus |
|
Related with Spinal lamniscus |
Present |
Present |
Absent |
|
Related with Medial lamniscus |
Absent |
Absent |
Present |
|
Destination |
Post central gyrus |
Post central gyrus |
Post central gyrus
|
|
Lesion |
Contra-lateral loss of pain and thermal sensibilities below the level of the lesion Unable to sense pin prick or recognize hot or cold objects |
Contra-lateral loss of light touch and pressure sensibilities below the level of the lesion. Discriminative touch will be present but unable to feel light touch of cotton placed against the skin |
Ipsilateral loss of muscle and joint sensation, two point discrimination and vibration below the level of lesion but sense of light touch is unaffected Movement are jerky or ataxic |
Wednesday, October 21, 2020
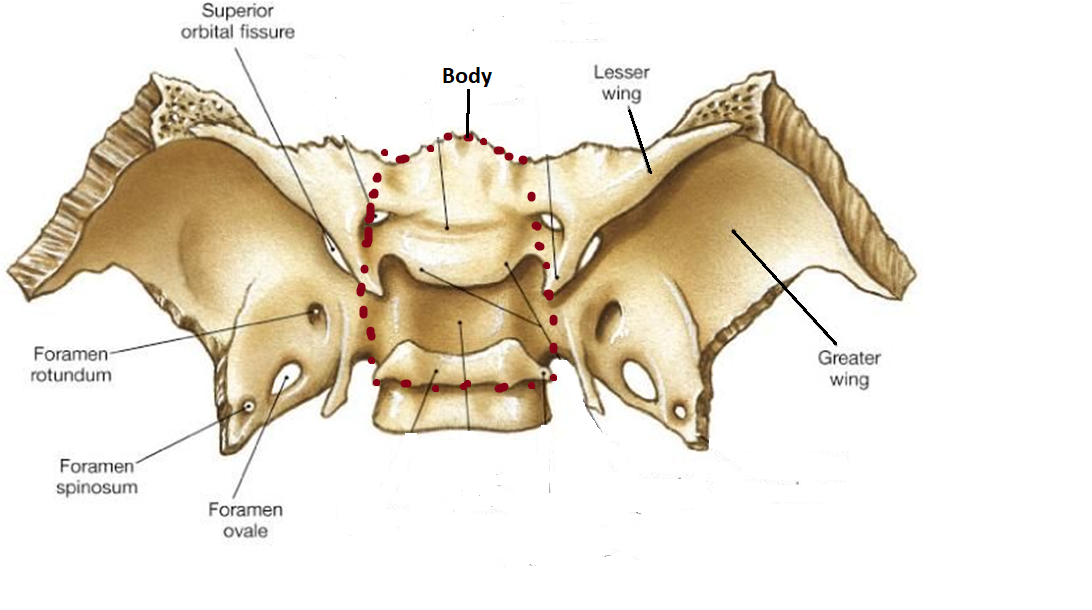
Anatomy of sphenoid
Anatomy of sphenoid
Anatomical points
- Body lies centrally
- superior surface of body lies horizontally
- Two greater wings & two lesser wings project laterally from the sides of the body
- Superior surfaces of greater wings are deeply concave
- Two pterygoid processes are directed downwards from adjoining parts of the body and greater wings Morphological type of bone: pneumatic irregular bone
https://www.amazon.com/gp/product/B08L7R9DL4/ref=as_li_tl?ie=UTF8&camp=1789&creative=9325&creativeASIN=B08L7R9DL4&linkCode=as2&tag=ezhumanatomy-20&linkId=e4dff7c8da8662c897ebe16b667f67f1
Parts of sphenoid bone
Body
Two greater wings
Two lesser wings
Two pterygoid processes
Body: It has six surfaces : superior , inferior , anterior , posterior and two lateral surfaces
Shape : cuboid
It contains two large air sinuses which are separated from each other by a septum
Superior or cerebral surface
Articulates with ethmoid bone anteriorly and basilar part of occipital bone posteriorly. It shows:
Ethmoidal spine : it is articulate with posterior border of cribriform plate of ethmoid bon
Jugum sphenoidale: smooth area which is the part of anterior cranial fossa . this part is related with gyri recti of cerebrum and olfactory tracts
Sulcus chiasmaticus: it is a groove which connects both optic canal . it lodges optic chiasm
Tuberculum sellae: round elevation it bears middle clinoid processe
Sella turcica: deep depression behind the tuberculum sellae . deepest part of sella turcica is
known as hypophyseal fossa
Dorsum sellae: square shape bone which form posterior boundary of sella turcica . it bear
posterior clinoid processes
Clivus: slopping area behind dorsum sellae . it continue with basilar part of occipital bone this part is related with pons
- Inferior surface
Rostrum of sphenoid
Sphenoidal conchae
Vaginal processes of medial pterygoid plate
Anterior surface
Sphenoidal crest articulates with the perpendicular plate of ethmoid leading to formation of a part of the septum of nose.
Posterior surface: Basilar part of occipital bone
Lateral surface
- It is united with the greater wing and medial pterygoid plate ,
Carotid sulcus is present in the lateral surface which is extend from superior orbital fissure to foramen lacerum s lodging cavernous sinus and internal carotid - Development:
- up to rostral half of sella turcica is developed from neural crest
- caudal half of sella turcica is developed from paraxial mesoderm

{kind=link}

Thursday, October 15, 2020
Difference between arteriole and
venule
|
Arteriole
|
Venule
|
|
Arterioles distribute blood to capillary beds, the sites of
exchange with the body tissues. |
Blood of capillaries
lead back to small vessels known as venules that flow into the larger veins
and eventually back to the heart. |
|
·
The lumina of arteriole are much
smaller than corresponding venule |
·
The lumina of venules are much
larger than corresponding arterioles.
|
|
·
It is also known as
resistance vessel |
It is also known as
capacitance vessel |
|
·
The walls of the arteriole are much
thicker than venule |
·
The walls of the veins are much
thinner than arterioles |
|
Arteriole
provides 50% peripheral resistance |
·
Veins and venules can withstand a
much lower pressure from the blood flowing through them. Their lumens are correspondingly
larger in diameter to allow more blood to flow with less vessel resistance.
|
Monday, October 12, 2020
Arteriole : lecture note
Arteriole
The greatest change in blood pressure and velocity of blood flow occurs at the transition of arterioles to capillaries. An arteriole is a small-diameter blood vessel in the microcirculation that extends and branches out from an artery and leads to capillaries
Arteriole is also known as resistance vessels . Most arterioles can dilate 60% to 100% from their resting diameter, and they can maintain as much as 40% constriction for a long time. Therefore, a large decrease or increase in vascular resistance has a direct effect on distribution of blood flow and systemic arterial pressure.
Arteriole About 10 percent of the total blood volume is in the systemic arterial system at any given
If all the arteries, veins, and capillaries were laid end to end, the total length would be 100,000 km
The diameter of arterioles are in between 100 to 300 µm.
Arteriole: Like any other blood vessels arteriole is made by three concentric layers (within outward )
Tunica intima ,Tunica media and Tunica adventitia
Tunica intima of arteriole contain
1. endothelium & its basement membrane
2. Subendothelial connective tissue is formed by loose connective tissue which contain smooth muscle cells
3. Large arteriole contain internal elastic lamina but small arteriole contain no internal elastic lamina
Tunica media of arteriole contain Circularly arrange smooth muscle cells layers(1-2 cells layer) with variable amounts of elastin, reticular fibers, and proteoglycans are interposed between the smooth muscle cells
Arteriole has tunica adventitia which is composed of collagenous & elastic connective tissues, whose thickness approaches that of the tunica media.
Large arteriole contain external elastic lamina but small arteriole contain no external elastic lamina
Arterioles control blood flow to capillary networks by contraction of the smooth muscle cells. Arterioles serve as flow regulators for the capillary beds. In the normal relationship between an arteriole and a capillary network, contraction of the smooth muscle in the wall of an arteriole increases the vascular resistance and reduces or shuts off the blood going to the capillaries.
Arteriole is also known as resistance vessels . Most arterioles can dilate 60% to 100% from their resting diameter, and they can maintain as much as 40% constriction for a long time. Therefore, a large decrease or increase in vascular resistance has a direct effect on distribution of blood flow and systemic arterial pressure.